Why is it important for health systems to focus on post-acute care today?
How can health systems reinvent their post-acute care models to succeed in risk-based models?
What must health systems do to drive higher performance in their facilities and better outcomes for their patients?
In this episode of Navvis’ Take 5 podcast Senior Vice President of Care Networks at Navvis, Kristi Short explains the changes that post-acute care is going through.
Listen in on this discussion between Kristi and Chuck Eberl, Navvis’ Chief Strategy Officer, to find out why health systems must focus on post-acute care. The transcript is below, lightly edited for length and clarity. You can also access the audio for all Navvis Take 5 episodes here.
To start off, can you give us some background on what’s been happening in post-acute care, and why this is such an important area for health systems to be focused on?
Kristi Short: This is a great, interesting transitional time for post-acute care. Over the last couple of decades, it’s moved from the shadows into the spotlight, and a lot of things are going on to level set.
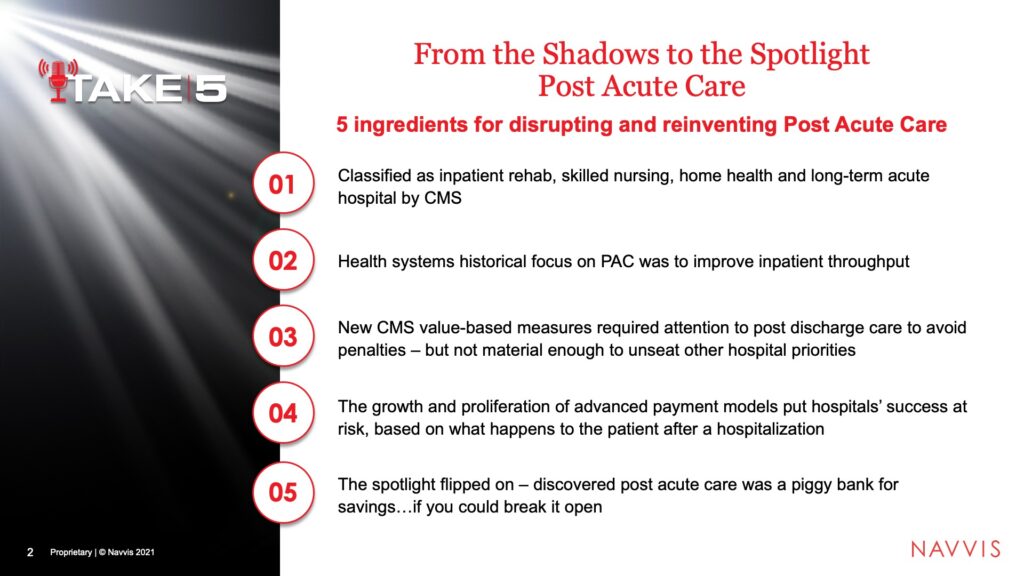
When we talk about post-acute care, we use the CMS (Centers for Medicare & Medicaid Services) definition, which is inpatient rehab, skilled nursing, home health, and long-term acute care. Those are the venues that are wrapped in. Historically, when I started out focusing on post-acute health systems, we were only looking at them because they needed a place to put their patient from hospitalizations quickly. The focus was on the patient throughput. Then the CMS value-based measures came along, and readmission penalties came along, but that wasn’t enough. They weren’t material enough to unseat other hospital priorities. So it stayed a little bit in the shadows until now.
The growth of advanced payment models put hospital success in those models at risk if they did not attend to post-acute care. What happens to the patient when they leave the hospital became very important. It’s like a spotlight flipped on and they discovered post-acute care is really the first level, the first piggy bank for savings, because of the large variation of what happens to the patient when they leave the hospital.
What I tried to think about for our audience today is: After these 20 years, what are the five ingredients that we have found for disrupting and reinventing your post-acute care model so you can be successful in risk-based advanced payment models?
What are those five ingredients?
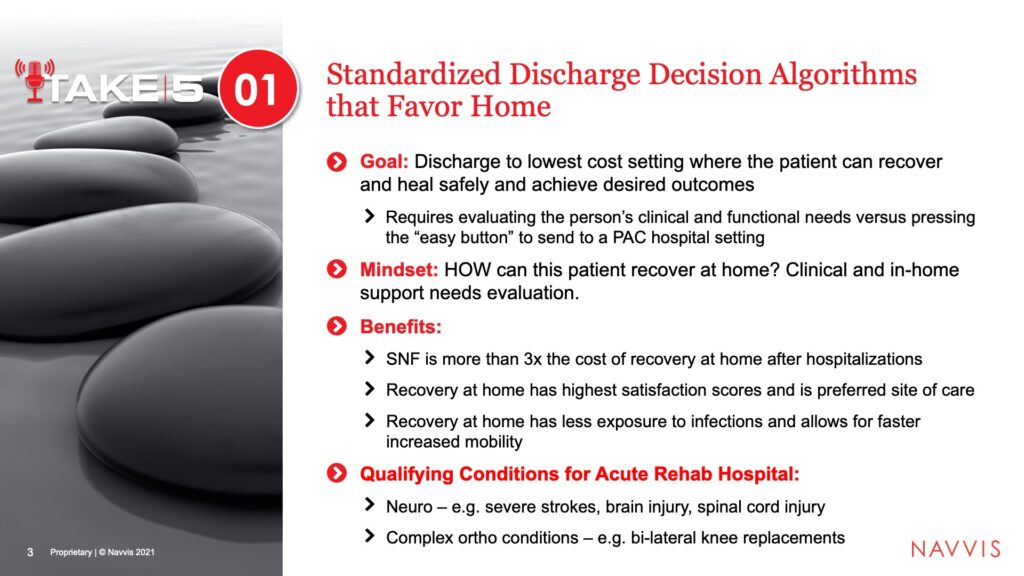
Let’s start with number one. One of the most important areas is standardized discharge decision algorithms. That’s a mouthful, but what that basically means is getting the patients to the next venue of care that is the lowest cost setting where the patient can recover and heal safely.
Many times, we find that hospitalists and other physicians use what we call the easy button and send patients to SNFs (skilled nursing facilities) because then they don’t have to worry about making sure the home environment is set up correctly. They know that the patient will be cared for with skilled nursing facilities. But to send the patient to skilled nursing is nationwide about $14,000, $15,000. It’s a major decision, especially if you’re participating in an MSSP (Medicare Shared Savings Program).
The mindset needs to be, how can this patient recover at home? What are the clinical needs? What are the in-home support needs? Take the time and evaluate those and get them home if possible.
There are multiple benefits for the patient going home. SNF costs three times as much for recovery. At home is more and more where patients want to recover because of reduced risk of infection and a whole host of other reasons. The invention of telemedicine technology allows for consults in the home.
We do know that there will always be a place for higher acuity rehab hospitals, for catastrophic conditions like brain injury, spinal cord injury, or severe strokes, when patients need the intensity that only an inpatient rehab hospital can provide. But you have to be very discerning when you send a patient to inpatient rehab, which can be tricky, especially with our health systems who own inpatient rehabs because they’re quite profitable. At the same time, the average cost of going to an inpatient rehab could be upwards to $25,000. If that person can recover in a SNF (Skilled Nursing Facility) or even more at home, it’s better for the success of the contract and better for the patient.
Once you decide someone’s going to a skilled nursing facility, how do you get them to the right provider?
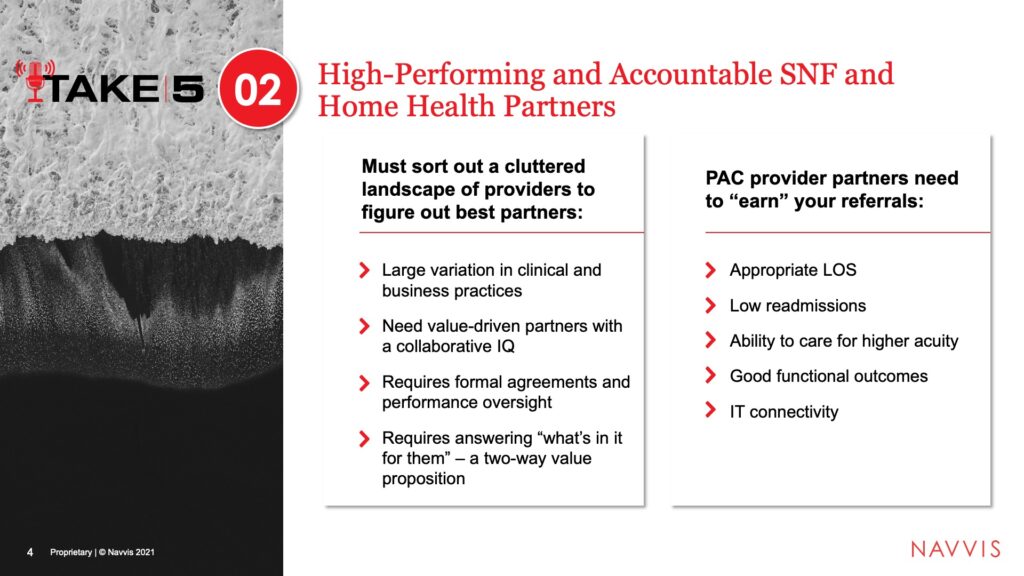
That is number two on our list of five today, and that is building high performing and accountable skilled nursing and home health partner networks. You must really sort out what’s a very cluttered landscape and the types and variation of service that is provided in your communities by your home health agencies as well as your skilled nursing facilities. You need to find partners that are value-driven, partners with what we call a collaborative IQ. They want to partner with you and have your interest in mind.
This really requires sorting them out based on performance measures and putting them under a formal agreement that includes metrics that they have to hit to maintain the status in your preferred network. Because if you put them in a preferred network, it’s really an extension of your brand. They’re part of the family.
We also know that it requires a two-way value proposition. There has to be value for them to comply with reducing length of stay, to do everything they can to lower readmissions, to build up their capabilities to care for higher acuity. There are a lot of asks you are going to have of them to be part of the preferred network, so there has to be a value proposition for them in the equation.
This is a very vulnerable time for skilled nursing facilities and home health because they are being pushed to care for high acuity that they’ve never had to care for before. Health systems have the assets to help them, and that is the value proposition. In addition, of course, they are very dependent on referrals. With unprecedented consolidation in this whole post-acute industry, never before have they really wanted to lock up their referral channels. This is the right time for change in that regard.
Once the patient is in the post-acute network, how do you follow them through the continuum and make sure that they actually get home?
We have the discharge decision algorithm that gets them to the right location when possible. If they need to go to a skilled facility or home health, we have vetted a group of partners, so we get them to the right partner.
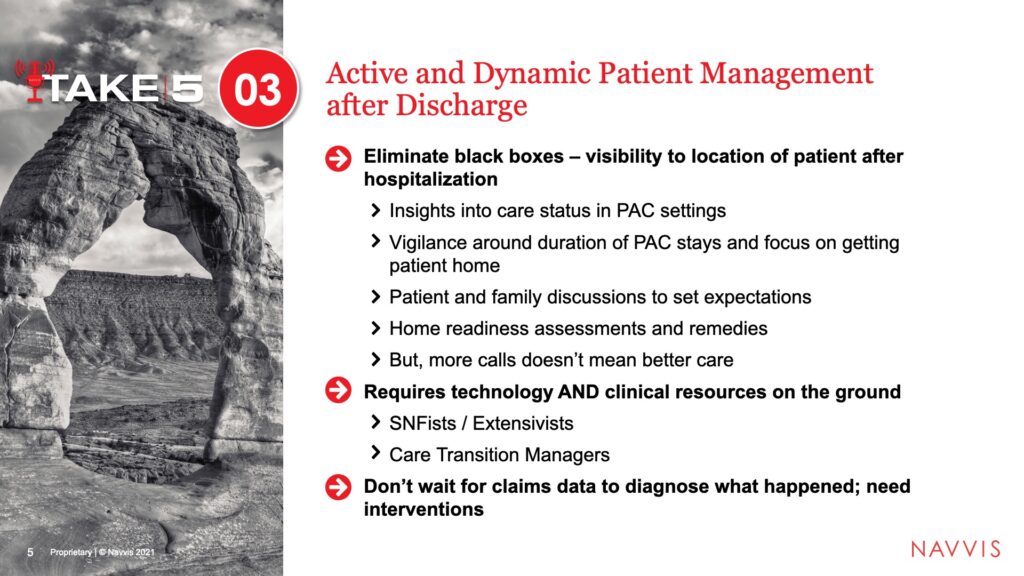
We need to manage that patient as they go through the continuum and eliminate what we’ve seen as black boxes, where post-hospitalization, you don’t know where the patient goes. You don’t know what’s happening to them. You’ve taken all of this great care while they’re here and then you just send them somewhere.
You have to have the technology in place to know where they are at any given time, how long they’ve been there, and when they are going to be discharged. You have to have interactions with the family and with the patient to set expectations. You’re trying to get them out of the facility as soon as possible to reduce the cost of that stay, but you want to get them home for many other reasons, which we talked about. So you need to do a home readiness assessment. Are the paths clear? Are the lights adequate? Are there bars in the bathrooms? Are the things set up to aid in their recovery?
And the last thing is, if health systems have some patients being called by multiple departments when they’re discharged, more calls are not always better because then they can quit answering. You have to organize internally to make sure you know who’s calling the patient and not have multiple mixed messages to the patient. That’s key.
The other thing is boots on the ground. We find that the most successful organizations that manage post-acute follow the patient into the skilled nursing setting and ensure a timely discharge. They have care transition managers on the ground, or at least available via phone or video phone, to follow the patients as well, to get them out and safely to their home. You don’t want to wait three months later until you get the claims statement to see what happened — that a person went to three different post-acute facilities and the whole cost of that episode was $100,000. You want to be able to intervene and do things while that patient is moving the continuum to secure your success in these risk-based contracts.
How should health systems who own post-acute facilities think about this work as they’re trying to drive higher performance in their facilities and for their patients?
Back in the nineties, a lot of health systems sold their post-acute assets and focused just on hospitals. Those that kept them are very happy right now because they are able to own the care continuum where the patient is being seen. However, what we find is many times those post-acute assets have been operating in a silo and haven’t really been integrated into the value-based equation.
My advice is to reintroduce yourself to your home health agencies, to your skilled nursing facilities, to your inpatient rehab assets and the leadership. Give them an actual seat at the strategic table of how you’re going to put the pieces together to the benefit of the patient and to the benefit of your performance. We know that sending patients to your own facilities is the best way to manage them because you’re managing the performance of the facility.
Usually you’re on connecting or on the same EMR (electronic medical record), so this is the best way to control them. By the way, you’d get the revenue instead of sending them out to the competition. Home health agencies, if you’re so fortunate to have home health agencies at this time, are just foundational to moving more care into the home. There’s really a turf war going on in the home. You’ve got all of this new money flowing in to own the patient’s home and get a piece of the healthcare dollar.
My message there is, don’t leave this space. The home is the future of healthcare. It’s so important, and you need to be innovative and agile with your home health agencies. Dust them off, shine them up, and put them to work in this new environment.
What are the lessons learned, and what are the challenges that people face? What are some key takeaways you can offer us?
I can’t say it’s going to be easy. This is hard stuff, and you will face a lot of challenges, none of which can’t be overcome. They are formidable challenges. There’s a long history of the way that physicians and hospitals have done things, but it is absolutely worth it because if you think about it, 40% of the cost of an episode is incurred when the patient leaves. Managing that patient with strong post-acute relationships is critical, but expect to run into conflicts like physician loyalty and alignment, medical directorships, and so on.
Post-acute providers and those providers that have longstanding relationships may not be the best ones for your future. You have to deal with that. You’ll have to wean your organization from dependency that you may have. I alluded earlier to inpatient rehab profitability. If you own or are in a joint venture of those assets, LTAC (long-term acute care) and rehab profit margins are pretty healthy, many times in the 20 to 25%. But when you send those patients to inpatient rehab, you may be getting a profit margin but hurting yourself in value-based performance. You have to balance that out.
Another area would be the case managers and the SNFists. You need to get them on board. They are critical stakeholders. The case managers that have been in this business a long time may be very concerned about what we call using informed choice to drive referral to the preferred providers because Medicare does require choice. They may be concerned about putting in front of the patient a preferred provider list versus just giving them the list of all of the SNFs they can choose from. You have to get over that hurdle. CMS has loosened the requirements in that regard.
Then you have the hospitals and SNFs that have traditionally been rewarded on the volume of patients treated, not on the outcomes, not how quickly they get them out of the hospital or safely home. You have to look at those contracts and make sure they’re aligned with what you’re trying to accomplish.
The last thing is home-based health agencies. This is such a gem if you happen to have that in your portfolio, but if they’ve operated at the hospital-based home agency for a long time, they might have a little difficulty building some muscle, the ability to flex and embrace innovation to compete with these new agile entrants into the marketplace.
About Kristi Short
Kristi Short is Navvis’ Senior Vice President of Care Networks. A national expert in post-acute care and care networks, Kristi has over 20 years of experience in healthcare helping clients ensure the successful design and delivery of care management and population health programs.